







-
Diabetes during pregnancy poses a significant public health concern, due to its association with adverse maternal and offspring outcomes[1]. Globally, diabetes affects 21.1 million births (16.2%), with gestational diabetes mellitus (GDM) accounting for 80.3%, followed by 9.1% type 1 diabetes (T1DM) or type 2 diabetes (T2DM) first detected during pregnancy, and 10.6% pregestational T1DM and T2DM[2]. The rising prevalence of diabetes in pregnancy has been attributed to factors such as advanced maternal age, increasing obesity rates amongst women of reproductive age, and a family history of diabetes[3−5]. Increasing evidence has linked diabetes in pregnancy with pregnancy complications, including preeclampsia, emergency caesarean delivery and infections in mothers, while perinatal complications include preterm birth, macrosomia, shoulder dystocia, and respiratory distress syndrome in offspring[6−8]. Although evidence suggests that these adverse outcomes are more severe in women with pregestational diabetes compared to those with GDM, the underlying pathophysiological mechanism is not yet completely understood. Thus, understanding the mechanisms that link different types of diabetes with pregnancy and birth complications are critical in preventing adverse maternal and offspring health outcomes.
According to the 'Developmental Origins of Health and Disease' hypothesis, unfavourable exposure during crucial developmental periods, particularly during pregnancy and early childhood, may increase susceptibility to chronic diseases in later life[9]. Offspring of women with diabetes during pregnancy are exposed to a hyperglycaemic intrauterine environment, increasing their risk of developing metabolic diseases such as obesity, T2DM, and cardiovascular disease[10−12]. However, identifying pregnancies at high risk of adverse outcomes remains a significant challenge due to limitations in current screening and diagnostic methods. Epigenetics, particularly DNA methylation, have emerged as a potential mechanisms linking maternal diabetes to short- and long-term health effects[13]. DNA methylation is the most widely studied epigenetic mechanism that involves the addition of a methyl group to the C5 position of the cytosine ring within the nucleotide sequence[14]. DNA methylation is known to regulate gene expression and has been shown to influence various cellular processes such as development, differentiation, and genomic stability[15]. Recent studies suggest that DNA methylation plays a role in the physiological adaptations that occur during pregnancy[16], and its dysregulation has been associated with pregnancy complications such as preeclampsia, hypertension, preterm birth, and birth weight in placental tissue, and maternal and cord blood[17−21]. Additionally, several studies have reported alterations in global DNA methylation associated with hyperglycaemia in peripheral blood[22−24], and in placental tissue and cord blood of women with GDM[25−27], thus offering the potential for maternal blood DNA methylation to serve as an early indicator of adverse pregnancy and birth outcomes in high-risk pregnant women.
To date, no study has explored the association between global DNA methylation in maternal blood and birth outcomes in women with diabetes in pregnancy within a South African population. Global DNA methylation provides an overview of methylation changes across the genome, allowing researchers to capture broad epigenetic changes rather than focusing on specific individual loci. Moreover, global methylation offers a cost-effective and minimally invasive approach, making it attractive for biomarker discovery and a valuable screening tool for the early detection of high risk pregnancies. The aim of this exploratory study is to investigate the association between global DNA methylation and birth outcomes in South African women with different types of diabetes in pregnancy. Global DNA methylation was quantified in peripheral blood samples of 230 pregnant women with T1DM (n = 26), T2DM (n = 77), GDM (n = 58), and normoglycemia (n = 69), using the Imprint Methylated DNA quantification kit. Associations between global DNA and diabetes type, maternal characteristics, and birth outcomes were analysed.
-
Pregnant women with and without diabetes, attending the diabetic antenatal clinic at Steve Biko Academic Hospital, Pretoria, South Africa, were recruited to the study between May 2017 and April 2023. Of the 230 women requested to participate in the study, only five declined (response rate: 97.8%). Eligible participants were women between the ages of 18 and 40 years, self-reported black African, less than 28 weeks gestation, and human immunodeficiency virus (HIV) negative. Women who had a multiple pregnancies or whose fetuses had congenital abnormalities were excluded from the study. Written informed consent was obtained after participants were informed about the study's aims and procedures, and all collected data was anonymised to ensure confidentiality.
Maternal clinical and metabolic characteristics
-
A total of 230 pregnant women with T1DM (n = 26), T2DM (n = 77), GDM (n = 58) and normoglycemia (controls) (n = 69), were included in this exploratory study. T1DM and T2DM, referred to as pregestational or pre-existing diabetes, were based on self-report and medication history. Women without a history of pregestational diabetes underwent a 75-g 2-h oral glucose tolerance test (OGTT) between 24−28 weeks gestation, as recommended by Internation Association of Diabetes in Pregnancy Study Group (IADPSG), 2010[28], and the World Health Organization (WHO), 2013[29] diagnostic criteria. At recruitment, a standardized questionnaire was used to collect clinical and demographic data, including general medical and family history of diabetes. Anthropometric and demographic measurements, including age (years), body weight (kg), and height (m), were recorded according to the clinic's standard operating procedures, and body mass index (BMI) was calculated as weight (kg)/[height (m)]2. Categories for BMI were defined according to the Institute of Medicine guidelines[30] as normal weight (BMI = 18.5–24.9 kg/m2), overweight (BMI = 25.0–29.9 kg/m2), and obese (BMI ≥ 30 kg/m2). Fasting whole blood and serum samples were collected by venipuncture and stored at −80 °C until further analysis. Whole blood was used for DNA methylation profiling, while serum samples were analysed for circulating levels of insulin, C-peptide, total and high molecular weight (HMW) adiponectin, C-reactive protein (CRP), and triglycerides (TGs) using commercial enzyme-linked immunosorbent assays (ELISAs), according to the manufacturer's instructions (Merck Millipore, Massachusetts, USA).
Neonatal clinical characteristics
-
Neonatal outcomes were recorded at birth according to standard clinical procedures. Data on fetal growth, birth weight, offspring sex, 5 min Apgar score, and gestational age (GA) at delivery were collected. Fetal growth was categorized as small for gestational age (SGA, < 10th percentile), appropriate for gestational age (AGA, 10th and 90th percentile), and large for gestational age (LGA, > 90th percentile)[31]. Preterm birth was defined as delivery before 37 weeks gestation. Women who delivered prematurely were stratified according to early preterm (< 34 weeks gestation) and late preterm birth (34 to < 37 weeks gestation). Birth weight categories were defined as low birth weight (501−2,500 g), normal weight (2,500−4,000 g), and macrosomia (> 4,000 g), as previously defined[32]. Apgar score at 5 min was categorized as low if it was < 7 and as normal if it was ≥ 7.
Global DNA methylation profiling
-
Genomic DNA was extracted from 2 ml of whole blood using the QIAmp DNA Blood Midi Kit (Qiagen, Hilden, Germany). DNA concentrations were assessed with the Qubit Fluorometer and the dsDNA Broad Range Assay Kit (Invitrogen, Carlsbad, USA). Global DNA methylation was measured using the MDQ1 Imprint Methylated DNA quantification Kit (Sigma-Aldrich, St. Louis, USA), according to the manufacturer's protocol. Briefly, 50 ng of DNA was bound onto the ELISA plate, and the methylated DNA fraction was detected using a 5-methylcytosine monoclonal antibody. Quantification was performed colorimetrically by measuring the absorbance at 450 nm on a SpectraMax® i3x plate reader (Molecular Devices, California, USA). Each sample was analysed in duplicate, and global DNA methylation levels were determined relative to the 50 ng methylated positive control provided in the kit.
Sample size and power consideration
-
This exploratory study aimed to investigate the novel association between peripheral blood global DNA methylation and birth outcomes in pregnant women with different types of diabetes. While no prior data or literature exists to reliably estimate effect sizes specifically exploring this relationship, a priori power analysis was not conducted. This is typical for hypothesis-generating studies where the primary goal is to identify potential associations rather than provide confirmatory evidence, as highlighted in recent literature[33].
Statistical analysis
-
Statistical analysis was performed using STATA 14 (StataCorp, College Station, TX, USA) and graphs were created using Prism 7, Version 7.03 (GraphPad, La Jolla, USA). Normality was assessed using the Shapiro-Wilk test. Exploratory analyses were performed using histograms, bar graphs, and box plots, and outliers were confirmed using GraphPad outlier calculator software (
www.graphpad.com/quickcalcs/grubbs1 ) and removed from the analysis where appropriate. Normally distributed data (parametric) were expressed as mean ± standard error of the mean (SEM), while non-parametric data were expressed as the median and interquartile range (25th−75th percentile). For comparisons across more than two groups, one-way ANOVA with Holm-Sidak's multiple comparisons test was used for parametric data, and Kruskal-Wallis with Dunn's test for non-parametric data. For comparison between two groups, the unpaired Student's t-test was used for parametric data, while the Mann-Whitney test was used for non-parametric data. Categorical data were expressed as count (n) and percentage (%) and analysed using the Chi-squared test or the Fisher's exact test when frequencies were < 5. To assess the association between global DNA methylation and clinical and metabolic characteristics, Spearman's correlation was performed. For further analysis, women with pregestational T2DM and newly diagnosed T2DM were grouped under the assumption that newly diagnosed cases represented undiagnosed pre-existing T2DM and showed no significant differences in biochemical markers. To evaluate the ability of DNA methylation and other factors to predict preterm birth, discriminant, and receiver operating characteristic (ROC) curves were conducted, and the area under the curve (AUC), sensitivity, and specificity were determined using JMP software, Version 18.0.2 (SAS Institute Inc., Cary, NC, USA). Univariable and multivariable logistic regression models were used to assess the associations between global DNA methylation (continuous independent variable) and preterm birth (binary dependent variable), adjusting for confounders, such as age, BMI, and GA. A p-value of < 0.05 was considered statistically significant. -
The clinical characteristics of the study population are summarised in Table 1. Participants were stratified into pregnant women with normoglycemia (controls) (n = 69), preexisting T1DM (n = 26) and T2DM (n = 53), T2DM diagnosed for the first time during pregnancy (n = 24) (new T2DM), and GDM (n = 58). Women with T2DM and GDM were older than women with T1DM and controls, while BMI and body weight were increased in women with GDM compared to women with T1DM, T2DM, new T2DM, and normoglycemia. As expected, women with pregestational T1DM and T2DM visited the antenatal clinic earlier in their pregnancies and had elevated glycated haemoglobin (HbA1c) levels compared to women with new T2DM and GDM. In addition, women with new T2DM had higher 2 h glucose concentrations compared to women with GDM and the control group. Furthermore, women with T2DM and GDM had a history of hypertension compared to controls.
Table 1. Clinical characteristics of study participants.
Variable Controls T1DM T2DM New T2DM GDM p-value N 69 26 53 24 58 Age (years) 31.0 (27.0−36.6)a,b 29.0 (27.0−32.0)c,d 36.0 (30.0−37.0)a,c 33.5 (30.0−36.0) 35.5 (32.0−38.0)b,d <0.001 BMI (kg/m2) 31.7 (27.6−39.4)a 28.3 (23.8−33.5)b 32.5 (28.8−37.9)c 30.3 (28.8−34.4)e 38.9 (32.8−43.7)a,b,c,e <0.001 Weight (kg) 82.2 (70.4−94.4)b 71.7 (60.4−84.9)e,d 84.8 (73.1−98.9)e,f 85.4 (75.0−93.4) 101.0 (85.0−112.7)b,d,f <0.001 GA at recruitment (weeks) 22 (20−25)e,a 16.5 (14−21)e,b,f 20 (16−22)d,h 25 (20−26.5)f,h 25 (24−26)a,b,d <0.001 HbA1c (%) 5.2 (5.0−5.4)b,d,c 9.3 (7.6−10.1)b,g,e 7.7 (6.5−9.3)d,i 6.9 (5.9−8.7)c,e,h 5.7 (5.4−6.1)g,i,h <0.001 0-h OGTT (mmol/L) 3.9 (3.7−4.3)b,d − − 7.5 (6.7−9.9)d,a 5.4 (5.1−6)b,a <0.001 1-h OGTT (mmol/L) 5.6 (4.4−6.8)b,d − − 12.8 (12.1−14.9)d,a 9.9 (8.2−11)b,a <0.001 2-h OGTT (mmol/L) 4.5 (5.1−6.5)b,d − − 12.6 (11.2−15.9)d,g 8.8 (6.7−9.5)b,g <0.001 History of hypertension in pregnancy (Yes) 4 (7.7)e,h 3 (5.77) 19 (36.5)e 8 (15.4) 18 (34.6)h 0.001 All data are expressed as the median (25th–75th percentiles). p-values were calculated using the Kruskal Wallis test and Dunn's multiple comparisons. Similar superscripts indicate statistical significance between groups: e,h p < 0.05, a,c,f p < 0.01, b,d,g,i p < 0.001. T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus; GDM, gestational diabetes mellitus; GA, gestational age; BMI, body mass index, HbA1c, glycated haemoglobin, OGTT, oral glucose tolerance test. Next, levels of insulin, C-peptide, total and HMW adiponectin, TGs, and CRP were measured in the serum of pregnant women with pregestational T1DM and T2DM, newly diagnosed T2DM, GDM, and normoglycemia. The maternal metabolic characteristics of the study population are summarised in Table 2. Significant differences in C-peptide levels, a marker of beta cell function and insulin secretion[34], were identified between groups, with lower levels observed in women with T1DM compared to women with GDM, T2DM, and normoglycemia. Total adiponectin levels showed notable differences between groups, with higher levels observed in women with normoglycemia and T1DM compared to women with GDM. Additionally, HMW adiponectin levels were significantly different between groups, with higher levels observed in women with T1DM compared to women with T2DM.
Table 2. Metabolic characteristics of study participants.
Variable Controls T1DM T2DM New T2DM GDM p-value Insulin (μU/mL) 6.9 (1.4−29.1) 22.1 (5.8−37.9) 19.3 (3.4−40.4) 8.9 (3.5−25.0) 21.7 (4.8−54.6) 0.2161 C-peptide (ng/mL) 1.7 (0.8−3.1)a 0.5 (0−1.2)a,b,c 2.0 (1.0−2.6)b 1.8 (1.0−2.4) 2.2 (1.4−4.0)c <0.0001 Total Adiponectin (μg/mL) 7.6 (4.5−12.3)d 8.5 (4.2−16.1)e 4.8 (3.7−8.2) 3.9 (3.4−6.9) 4.2 (2.9−7.6)d,e 0.0016 HMW Adiponectin (μg/mL) 4773 (1962−7247) 10,210 (4,182−15,710)f 1,547 (1,154−2,276)f 2,259 (1,246−4,604) 2,292 (1,131−4,483) 0.0076 Triglycerides (mg/dL) 311.4 (232.8−426.4) 314.9 (279.5−539.0) 327.3 (233.0−698.5) 416.5 (284.9−554.9) 361.9 (311.9−492.7) 0.3861 All data are expressed as the median (25th–75th percentiles). p-values were calculated using the Kruskal Wallis test and Dunn's multiple comparisons. Similar superscripts indicate statistical significance between groups: d,e,f p < 0.05, a,b p < 0.01, e p < 0.001, c p < 0.0001. T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus; GDM, gestational diabetes mellitus; GA, gestational age; BMI, body mass index, HbA1c, glycated haemoglobin, OGTT, oral glucose tolerance test. Global DNA methylation is associated with preterm birth
-
The association between global DNA methylation and fetal growth, birth weight, offspring sex, 5 min Apgar score, and preterm birth were assessed (Fig. 1a−e). Women who delivered prematurely had 1.6-fold lower methylation levels compared to those who delivered at full term (p = 0.019) (Fig. 1e). When stratified according to early and late preterm birth, a significant reduction in global DNA methylation levels (1.9-fold; p = 0.027) was observed in women who had late preterm births compared to women who delivered at full term (Fig. 2b), while no difference was observed between early preterm birth and term births (Fig. 2a). A trend towards lower global DNA methylation was observed in neonates with a 5 min Apgar score < 7 (p = 0.09) (Fig. 1d), an indicator of potential neonatal health issues[35]. Furthermore, no association between global methylation and fetal growth, birth weight, and offspring sex was observed (Fig. 1a–c).
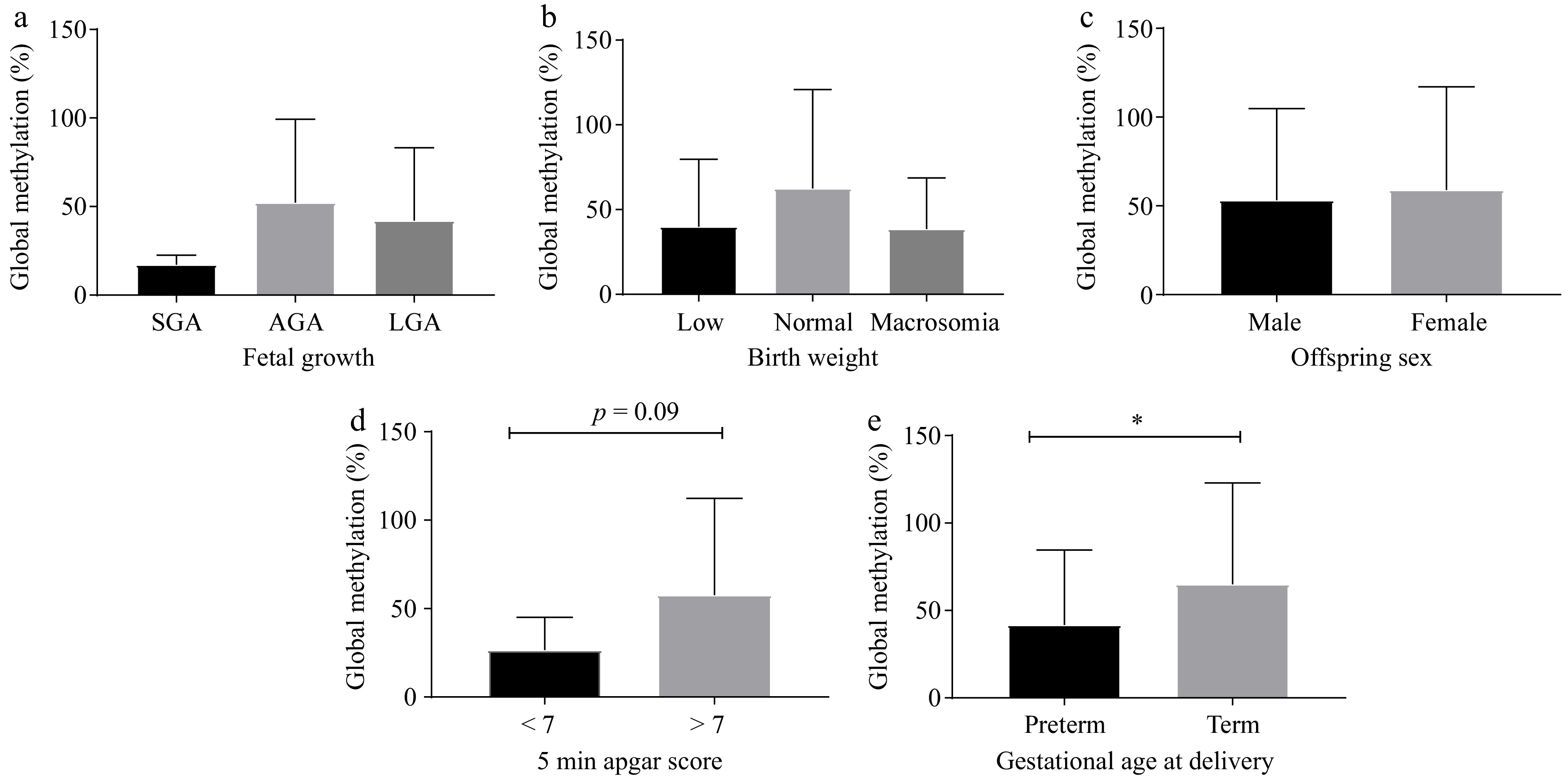
Figure 1.
Global DNA methylation is associated with birth outcomes. The percentage of global DNA methylation was compared with (a) fetal growth in utero, (b) birth weight, (c) offspring sex, (d) 5 min Apgar score, and (e) GA at delivery (n = 106−166). * p < 0.05. Abbreviations: GA, gestational age; SGA, small for gestational age; AGA, average for gestational age; LGA, large for gestational age; preterm birth: < 37 weeks gestation; term, full term: ≥ 37 weeks gestation.
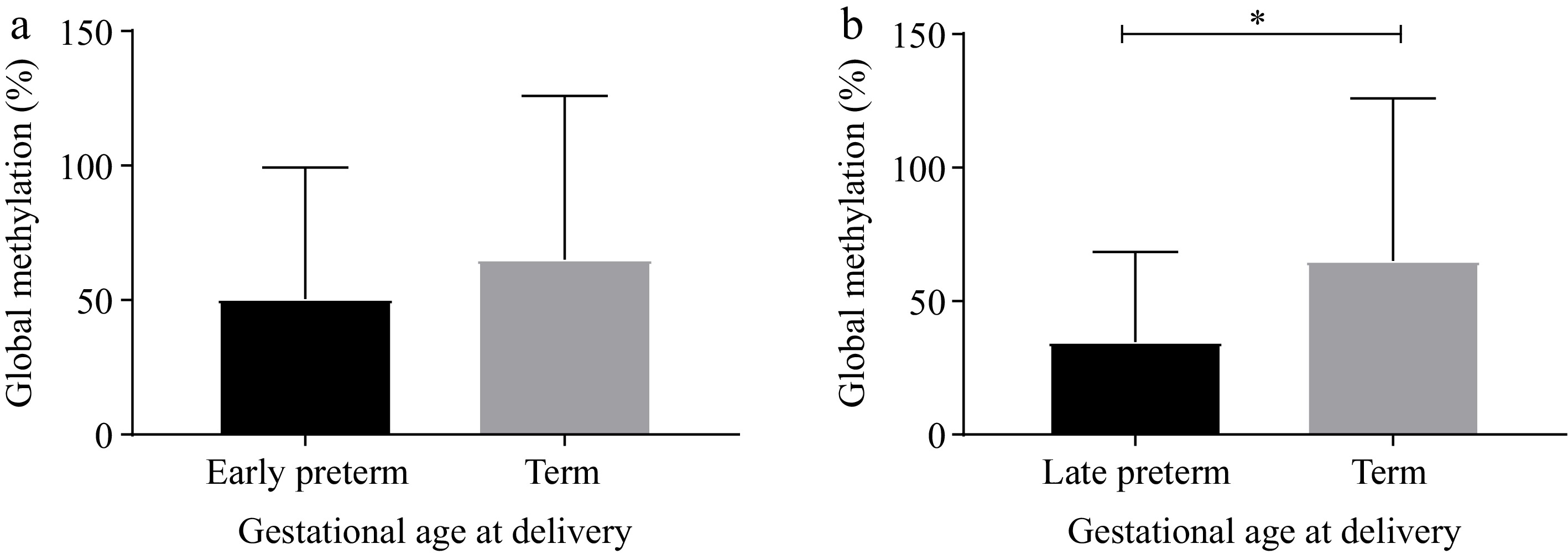
Figure 2.
Global DNA methylation stratified by early and late preterm birth. The percentage of global DNA methylation between (a) early preterm (20−33 weeks gestation) vs term births (37–40 weeks gestation), and (b) late preterm birth (34−36 weeks gestation) vs term births (37–40 weeks gestation). * p < 0.05.
Global DNA methylation varies according to maternal BMI
-
Spearman's correlation analysis showed no association between global DNA methylation levels and clinical and metabolic parameters (Supplementary Table S1). Since the extent of hyperglycaemia and BMI during pregnancy can influence methylation levels, global DNA methylation was analysed in women stratified according to T1DM, T2DM (including new T2DM), GDM, and normoglycemia, and according to normal weight, overweight, and obese (Fig. 3). No difference in global DNA methylation levels were observed between the different diabetes types (p > 0.05) (Fig. 3a). However, when stratifying according to BMI, women with obesity had 3.7-fold higher global DNA methylation levels compared to normal weight women (p = 0.025) (Fig. 3b).
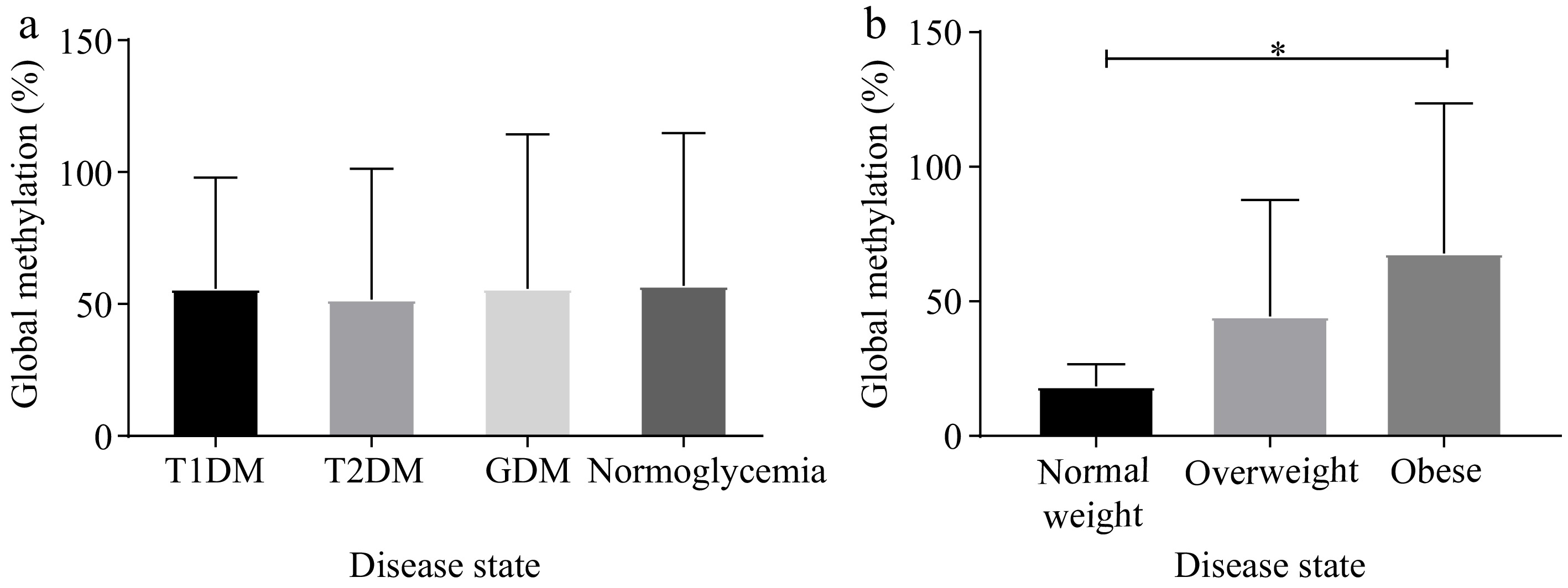
Figure 3.
Global DNA methylation differed according to obesity status not diabetes type. The percentage of global DNA methylation stratified according to diabetes or BMI categories. (a) Pregnant women with T1DM (n = 16), T2DM (n = 67), GDM (n = 39), and normoglycemia (n = 55), and (b) pregnant women with normal weight (n = 10), overweight (n = 33), and obesity (n = 85). *p < 0.05. T1DM: Type 1 diabetes, T2DM: Type 2 diabetes, GDM: gestational diabetes mellitus, BMI: body mass index.
ROC curve analysis was performed to evaluate the ability of global DNA methylation to predict preterm birth. Global DNA methylation showed modest discriminatory ability, with an AUC of 0.60, a sensitivity of 78.72% (95% CI: 64.34%−89.30%) and a specificity of 42.50% (95% CI: 33.53%−51.85%) in all women (Fig. 4a). When women were stratified according to BMI, global DNA methylation was able to better predict preterm birth in overweight and obese women with an AUC of 0.63, a sensitivity of 70.97% (95% CI: 51.96%−85.78%) and a specificity of 50.00% (95% CI: 39.02%−60.98%), compared to an AUC of 0.49 in normal-weight women (Fig. 5a & b). To evaluate whether a combination of global DNA methylation and other measured factors would improve the prediction of preterm birth, we performed multivariate discriminant and ROC curve analyses. The multivariate analysis revealed that a three-variable model incorporating global DNA methylation, HbA1c, and total adiponectin improved discrimination between preterm and term births with an AUC of 0.77, a sensitivity of 62.50% (95% CI: 40.59%−81.20%) and specificity of 76.09% (95% CI: 61.23%−87.41%) in all women (Fig. 4b) and an AUC of 0.78 a sensitivity of 63.16% (95% CI: 38.36%−83.71%) and specificity of 73.68% (95% CI: 56.90%−86.60%) in overweight and obese women (Fig. 5c), indicating better overall predictive performance compared to global DNA methylation alone, regardless of BMI stratification. Furthermore, in a regression model, the association between global methylation and preterm birth remained significant after adjusting for confounders, age, BMI, and GA (Table 3).
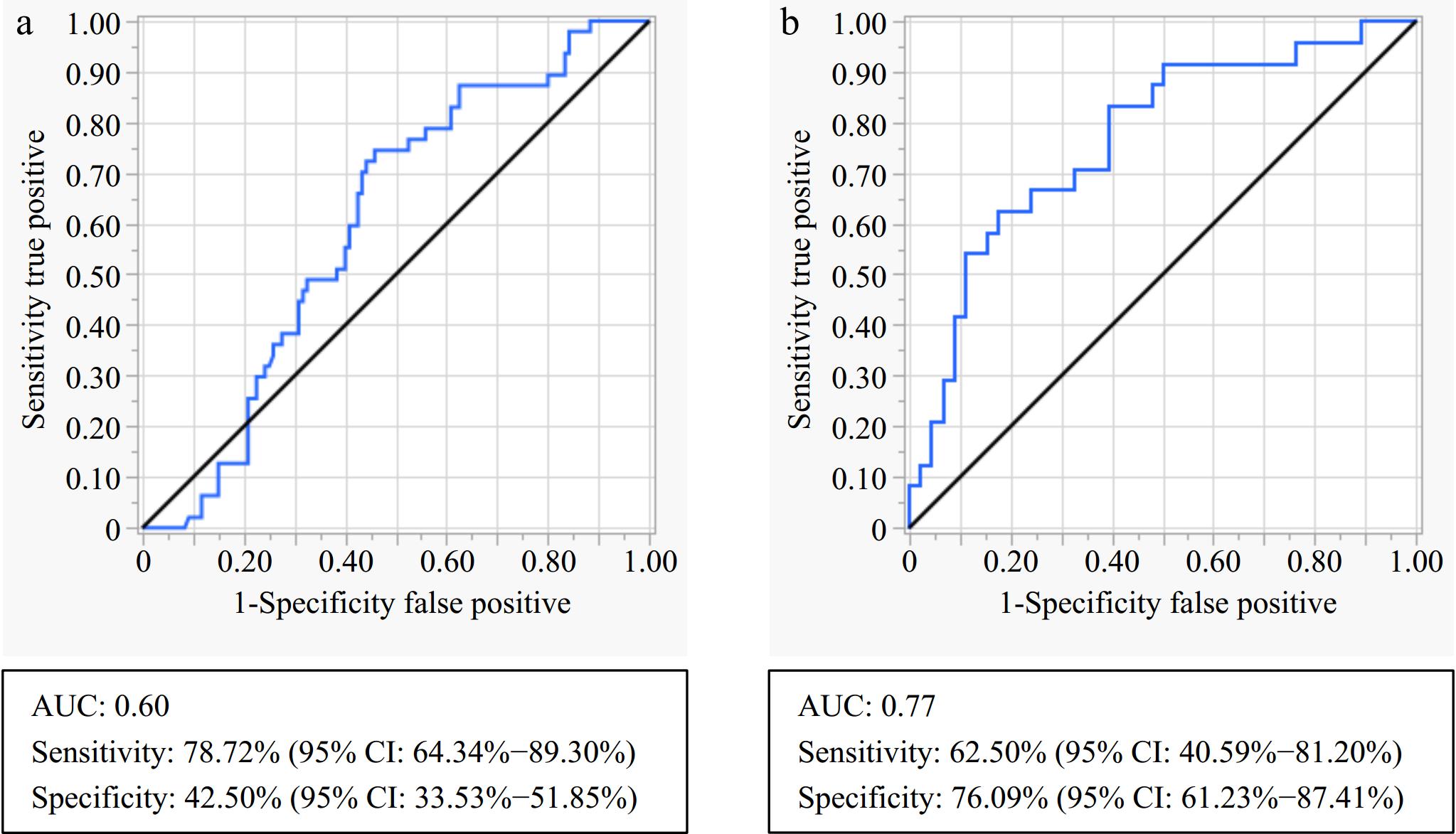
Figure 4.
ROC curve analysis for discriminating between preterm and term birth in all participants. (a) Global DNA methylation only, and (b) combined model of global methylation, HbA1c, and total adiponectin. ROC, Receiver operating characteristic; AUC, Area under the curve; HbA1c, glycated haemoglobin.
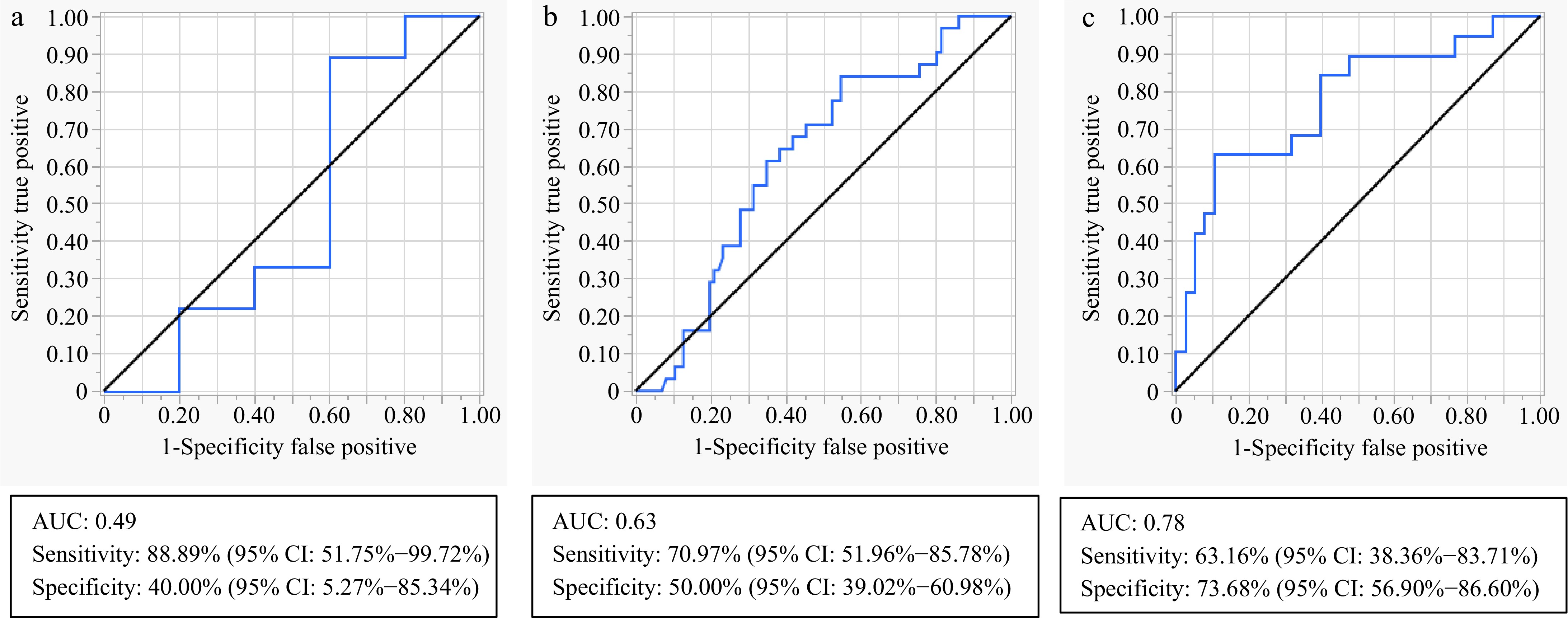
Figure 5.
ROC curve analysis for discriminating between preterm and term birth when stratifying according to BMI categories. (a) Global DNA methylation in normal weight women, (b) global DNA methylation in overweight and obese women, and (c) a combined model of global methylation, HbA1c, and total adiponectin in overweight and obese women. ROC, Receiver operating characteristic; AUC, Area under the curve; BMI, body mass index; HbA1c, glycated haemoglobin.
Table 3. Association between global DNA methylation and preterm birth.
Variable Model β co-efficient 95% CI p-value Global
methylation (%)Unadjusted model 0.328 0.046−0.611 0.023 Adjusted model 1 0.350 0.033−0.667 0.031 Adjusted model 2 0.428 0.079−0.776 0.016 Univariable regression analysis: Unadjusted model assessing the association between global DNA methylation and preterm birth. Multivariable regression analysis: Adjusted model 1: BMI; Adjusted model 2: age, BMI and GA. β, beta; CI, Confidence interval; BMI, body mass index; GA, gestational age. Statistical significance is indicated by p < 0.05. -
DNA methylation offers the potential to serve as a biomarker of adverse birth outcomes in high-risk pregnancies[19,20,26]. This study investigated the association between global DNA methylation in maternal blood and birth outcomes in South African women with diabetes during pregnancy. Our main findings showed decreased global DNA methylation levels in women with preterm births compared to those who delivered at full term. The association between global methylation and preterm birth remained significant after adjusting for confounding factors such as age, BMI, and GA. Moreover, a trend towards significance was observed between global DNA methylation and 5 min Apgar score < 7, an indicator of potential neonatal health issues[35], while no association between global DNA methylation and fetal growth, birth weight, and offspring sex were observed.
Global DNA methylation levels at ≤ 28 weeks of gestation were associated with preterm birth, with lower levels observed in women who delivered prematurely compared to those who delivered at term. The association between global DNA methylation and preterm birth was significantly strengthened after adjusting for confounders, age, BMI, and GA. Preterm birth is defined as delivery of a baby before 37 weeks of gestation and is a major contributor to neonatal mortality, accounting for approximately 7.2% of deaths in live births[35]. Preterm birth may also contribute to morbidity and an increased risk of long-term health complications such as cardiovascular disease, diabetes mellitus, kidney disease, and respiratory and neurological disorders[36−38]. Previously, studies have demonstrated an association between DNA methylation and preterm birth in maternal blood, cord blood, and placenta. However, research focused specifically on global methylation in maternal blood is limited, with only a few studies reporting an association[19,39−41]. Consistent with our findings, three studies showed an association between lower global DNA methylation levels and preterm birth[19,39,40]. Burris et al.[19], examined long interspersed nuclear element-1 (LINE-1), a surrogate measure of global DNA methylation levels[42], in maternal peripheral blood and demonstrated decreased first-trimester methylation in women who delivered prematurely[19]. The authors reported that the highest quartile of first-trimester LINE-1 methylation predicted a lower risk for preterm birth, while the lowest quartile of first-trimester LINE-1 methylation predicted a higher risk for preterm birth[19]. Another study, conducted by Chavan-Gautam et al., demonstrated decreased placental global DNA methylation in preterm deliveries among normotensive pregnant women compared to term pregnancies, using a Methylamp global methylation quantification kit[39]. Moreover, a study conducting LINE-1 methylation in mother-child dyads reported lower LINE-1 methylation levels in the cord blood of infants born prematurely[40]. These studies provide evidence for epigenetic similarities between maternal and fetal tissues, which may be key in determining whether maternal blood could be used as a marker for preterm birth. In our study, when women were stratified according to early and late preterm birth, global DNA methylation was lower in women with late preterm births compared to women who delivered at term, while no difference was observed between early preterm and term births. These findings were similar to those reported by Barišić et al., who showed no significant methylation differences in early preterm births in women who had spontaneous or emergency caesarean sections, compared to women with term births[41]. The lack of association observed may be due to the small sample size[41], or differences in the underlying mechanisms associated with early and late preterm births in these women. Furthermore, global DNA methylation showed a trend towards hypomethylation in offspring with 5-min Apgar scores < 7, compared to those with Apgar scores > 7. Apgar score is a measure of overall neonatal health at birth, with a score > 7 representing good neonatal health[43]. Previous research on preterm births demonstrated an increased risk of neonatal mortality as 5-min Apgar score decreased[44], providing biological plausibility for shared pathways amongst these adverse birth outcomes.
Higher global DNA methylation levels were observed in women with obesity compared to normal-weight women. The results observed were similar to our previous study showing increased global DNA methylation levels in a different cohort of South African pregnant women with or without obesity, regardless of GDM status[45]. The observed findings suggest that global DNA methylation changes may be induced by obesity-associated metabolic changes rather than changes in the degree of hyperglycaemia during pregnancy in this population. Obesity during pregnancy is considered a risk factor for maternal and birth complications, including, preeclampsia, gestational hypertension, GDM, preterm birth, and LGA at birth[46,47]. Global DNA methylation is widely reported to be associated with obesity[48−50], while studies in pregnant women with obesity are scant. Consistent with our findings, Nomura et al. observed increased global DNA methylation levels in the placenta of pregnant women with obesity compared to those with normal weight pregnancies, using the Luminometric methylation assays (LUMA)[26]. These findings indicate that maternal obesity may induce alterations in global DNA methylation within peripheral blood which may mirror changes observed in placental tissue, highlighting the potential of peripheral blood as a surrogate tissue for biomarker discovery during pregnancy.
ROC curve analysis revealed that global DNA methylation was better at predicting preterm birth in overweight and obese women compared to normal-weight women, while the three-variable model incorporating global DNA methylation, HbA1c, and total adiponectin, significantly improved the predictive ability of preterm birth regardless of BMI stratification. Evidence suggests that increased HbA1c and decreased total adiponectin serve as key markers of metabolic dysregulation during pregnancy and play a role in mechanisms such as oxidative stress, inflammation, insulin resistance, and placental dysfunction, contributing to adverse pregnancy outcomes[51,52]. These findings suggest that integrating global DNA methylation with metabolic markers such as HbA1c and adiponectin provides a more robust and generalizable predictive model for preterm birth, particularly in women with varying BMI and metabolic profiles. Incorporating these markers into predictive models could offer the potential for early risk stratification and targeted intervention strategies for high-risk pregnancies. However, further validation using data from diverse populations is needed to confirm and improve the predictive performance of these markers and ensure clinical applicability.
To our knowledge, this is the first study investigating the association between global DNA methylation and birth outcomes in South African women with diabetes in pregnancy. A notable strength of this study is the use of peripheral blood samples collected during pregnancy, which is minimally invasive and more readily accessible compared to other studies using cord blood and placenta[39,41]. However, this study is not without limitations. While peripheral blood offers several advantages for biomarker discovery in a clinical setting, it consists of a heterogenous cell composition with distinct DNA methylation patterns[53], which we did not adjust for in this study. Nonetheless, adjustment of cell type composition did not affect global methylation findings reported in other studies[54,55]. Additionally, the relatively small sample size in our study may have contributed to the lack of statistical power observed between diabetes groups. However, this exploratory study was designed to generate novel preliminary findings that can inform future research, thus, no formal sample size calculations were conducted, which is acknowledged as a limitation of this study. Moreover, while global methylation offers an overview of methylation differences, it may not provide insight into genes and pathways that play a role in the development of preterm birth. Thus, a more comprehensive approach such as whole-genome methylation profiling and gene-specific methylation studies[56] is needed to provide a better understanding of the mechanisms underlying preterm birth in this population. Furthermore, physical activity, dietary habits, smoking and alcohol consumption, which are all known influencers of methylation patterns[57−59], were not known for this study and could potentially confound our analysis. However, women recruited in this study were from the same community and had similar lifestyle behaviours, educational background, and socio economic and employment status, indicating that they had similar environmental influences.
-
In conclusion, these findings suggest that global DNA methylation in maternal peripheral blood, measured before 28 weeks of gestation, may serve as an early indicator of preterm birth in high-risk women. However, future longitudinal studies focused on gene-specific DNA methylation are required to elucidate the mechanisms underlying the development of preterm birth. Such studies may pave the way for targeted interventions or preventative strategies aimed at improving pregnancy outcomes.
The authors would like to thank the women who voluntarily participated in this study. This research was supported by funding from the National Research Foundation (NRF), Thuthuka funding (Grant No. 129844) to SD, the Competitive Programme for Rated Researchers (Grant No. 120832) to CP, and baseline funding from the South Africa Medical Research Council (CP).
-
This study was conducted in alignment with the Declaration of Helsinki, and ethical approval was obtained from the Human Research Ethics Committee of the University of Pretoria (protocol numbers 161/2016 and 743/2020). Written informed consent was obtained from all participants before their inclusion in the study. Participants were informed about the study's purpose, procedures, potential risks, and benefits, and their confidentiality was maintained throughout the research process. Data collection and analysis adhered to strict ethical guidelines to ensure participant privacy and data security. The study posed minimal risk to participants, and no identifying information was included in the final manuscript.
-
The authors confirm contribution to the paper as follows: study conception and design: Dias S, Pheiffer C; participant recruitment and sample collection: Adam S; data collection: Moloto P, Masete M; analysis and interpretation of results: Dias S, Mutavhatsindi H, van Niekerk J; draft manuscript preparation: Dias S. All authors reviewed the results and approved the final version of the manuscript.
-
All data generated or analysed during this study are included in this published article and its supplementary information files. The raw dataset used for the current study is available from the corresponding author on reasonable request.
-
The authors declare that they have no conflict of interest.
- Copyright: © 2025 by the author(s). Published by Maximum Academic Press, Fayetteville, GA. This article is an open access article distributed under Creative Commons Attribution License (CC BY 4.0), visit https://creativecommons.org/licenses/by/4.0/.
-
About this article
Cite this article
Dias S, Moloto P, van Niekerk J, Masete M, Adam S, et al. 2025. Reduced global DNA methylation in maternal peripheral blood is associated with preterm birth: an exploratory study in women with diabetes in pregnancy. Epigenetics Insights 18: e003 doi: 10.48130/epi-0025-0001 

Reduced global DNA methylation in maternal peripheral blood is associated with preterm birth: an exploratory study in women with diabetes in pregnancy
- Received: 29 August 2024
- Revised: 17 December 2024
- Accepted: 10 January 2025
- Published online: 03 March 2025
Abstract: Pregnancies complicated by diabetes pose a significant risk to maternal and neonatal health. Epigenetic mechanisms, particularly DNA methylation, have emerged as potential biomarkers for both pregnancy and birth outcomes. The aim of this exploratory study was to investigate the association between global DNA methylation and birth outcomes in South African women with different types of diabetes in pregnancy. Global DNA methylation levels were measured at less than 28 weeks of gestation, in peripheral blood samples of women with type 1 diabetes (T1DM, n = 26), type 2 diabetes (T2DM, n = 77), gestational diabetes mellitus (GDM, n = 58), and normoglycemia (n = 69), using the Imprint DNA quantification kit. Associations between DNA methylation and diabetes type, maternal characteristics, and birth outcomes were analysed. Women who delivered prematurely had 1.6-fold lower (p = 0.019) global DNA methylation levels compared to those who delivered at full term. This association remained significant after adjusting for confounders, age, body mass index, and gestational age (p = 0.031). A decreased trend towards significance was observed with 5 min Apgar score < 7 (p = 0.09), an indicator of overall neonatal health issues. No association between global DNA methylation and fetal growth, birth weight, and offspring sex were observed. These findings suggest that maternal global DNA methylation may serve as an early indicator of preterm birth in high risk women. Future studies focused on gene-specific DNA methylation are needed to elucidate the mechanisms involved in preterm birth.
-
Key words:
- Preterm birth /
- Global DNA methylation /
- Epigenetics /
- Diabetes in pregnancy /
- Fetal outcomes