









-
Colorectal cancer (CRC) represents the third most common cancer type and stands as the second leading cause of cancer-associated mortality globally[1]. Surgical and endoscopic resection remain the main curative options with a more than 90% 5-year survival rate, which depends on early diagnosis. In contrast, patients with advanced CRC face a significantly reduced 5-year survival rate of merely 10%, despite the recommendation of chemotherapy and various targeted agents[2−4]. For borderline curable CRC patients, surgery remains the preferred treatment approach. However, the majority of patients were diagnosed at an advanced stage and missed the opportunity for curative tumor resection. In addition, while adjuvant chemotherapy has presented to lower the risk of cancer recurrence, some postoperative CRC patients still experience disease relapse, resulting in limited overall survival (OS)[5,6]. To date, the underlying mechanisms and risk factors contributing to disease recurrence and patient outcomes remain poorly understood. Therefore, there appears significant interest in identifying critical biomarkers to predict outcomes in CRC patients, aiming to achieve accuracy management.
SYT8, a member of the calcium-sensitive family, has been demonstrated to facilitate the transport and cytosolization of secretory vesicles in non-neural tissues while inhibiting insulin efflux from permeabilized cells. Recent in vitro studies have indicated that suppressing SYT8 impedes the migration and invasion of gastric cancer cell lines[7,8]. In addition, overexpression of SYT8 has been significantly associated with peritoneal metastasis and was considered a valuable diagnostic and prognostic biomarker in gastric cancer patients[9−11]. Despite these findings, the clinicopathologic and prognostic significance of SYT8 in CRC patients remains unexplored.
In this study, we aimed to evaluate the diagnostic and prognostic potential of SYT8 utilizing CRC patient data from the TCGA dataset. To corroborate our findings, we conducted a retrospective analysis of CRC patients who received radical tumor resection at our center.
-
We downloaded colorectal cancer-related data from the TCGA-COADREAD dataset, including demographic information (gender, age, and race), clinicopathologic data (TNM stage, differentiation, body weight, height, and CEA level), survival follow-up, and SYT8 expression. Overall survival (OS) and progression-free interval (PFI) were calculated based on survival follow-up information and defined as the primary endpoints. The above data were organized via R software. We excluded the cases with incomplete follow-up data or lacking SYT8 expression. SYT8 core genes were identified online based on the Kaplan-Meier Plotter database (
http://kmplot.com/analysis ), and prognostic information was obtained for online analysis.The Affiliated Hospital of Nanjing University of Chinese Medicine's Ethics Committee approved this retrospective study (No. 2022NL-137-01), which analyzed 153 CRC patients treated at Jiangsu Provincial Hospital of Chinese Medicine between January 2016 and October 2020. All participants had a pathological diagnosis of adenocarcinoma and received curative tumor resection with lymph node dissection. We collected demographic, clinical, and pathological data, including age, gender, body measurements, tumor stage, margin status, and nerve and vascular invasion. Clinical staging was according to the 8th edition of the AJCC Cancer Staging Manual. We also collected formalin-fixed paraffin-embedded (FFPE) archival specimens. OS was calculated from the date of surgery to death from any cause, while disease-free survival (DFS) was measured from the surgical date to cancer recurrence confirmed by imaging or death. These endpoints were determined through telephone follow-ups or medical record reviews.
Inclusion and exclusion criteria
-
The inclusion criteria for this study were as follows: (1) pathologically confirmed colorectal cancer; (2) age range of 18−85 years; (3) radical tumor resection; and (4) ECOG score of 0−1. Exclusion criteria comprised: (1) presence of other primary malignant tumors; (2) unavailable pathology slides; (3) incomplete medical records; (4) death in one-month post-surgery; and (5) loss of follow-up.
Immunohistochemistry
-
Paraffin-embedded samples of CRC and adjacent tissues were carefully sectioned for slide preparation. The sections were hydrated, and antigen retrieval was performed utilizing citrate buffer. To minimize non-specific binding, the slides were treated with an endogenous peroxidase inhibitor and subjected to a 1-h serum block. Then, the sections were incubated overnight at 4 °C with an anti-SYT8 antibody (1:500 dilution, Abcam). Negative controls were prepared by substituting the primary antibody with PBS buffer. Following this, a secondary antibody (1:5000 dilution) was applied and incubated for 1 h at room temperature. The sections were then stained with DAB and counterstained with hematoxylin for 2 min. After dehydration, the slides were mounted utilizing neutral resin, and the immunohistochemical results were subject to an in-depth analysis under a microscope.
Two independent pathologists evaluated the slides, considering both the intensity of cell staining and the proportion of stained cells as scoring criteria. Consensus results were accepted, and in instances of discordance, the slides underwent re-evaluation. Staining intensity was graded as follows: 0 (no staining), 1 (weak staining, pale yellow), 2 (moderate staining, tan-yellow), and 3 (strong staining, brown). The cancer cell proportion was scored as 0 for positive cells < 10%, 1 for 10%−25%, 2 for > 25% and ≤ 50%, 3 for > 50% and ≤ 75%, and 4 for > 75%[12]. The final score, calculated by multiplying these two evaluations, was utilized to classify expression as either negative (< 4) or positive (≥ 4).
Statistical analysis
-
Statistical analyses were performed utilizing SPSS 25.0 and R software (version 4.2.3). For group comparisons, we employed the Wilcoxon signed-rank test or Student's t-test to evaluate variables between groups. The chi-square test was applied to appraise the relationship between SYT8 expression and clinicopathologic features. Survival analysis was performed by Kaplan-Meier assay and univariate analysis utilized Cox regression. Variables deriving p < 0.10 in univariate analysis were then incorporated into multivariate analysis. To ensure similar variable distribution between the training and validation sets, duodenal carcinoma patients were randomly allocated utilizing R software, with distributions compared through the Chi-square test or Fisher's exact test.
-
The analysis included 446 CRC patients, comprising 290 (65.0%) males and 93 (20.9%) Asians, with a mean age of 65.6 years. Patients were categorized into high-expression and low-expression groups based on median SYT8 expression levels. Interestingly, our findings indicated that SYT8 overexpression was only associated with the extent of primary tumor (p = 0.046) (Table 1). Further analysis of SYT8 expression levels in CRC and adjacent tissues demonstrated significantly higher expression in CRC tissues compared to adjacent tissues (0.84 ± 0.79 vs 0.28 ± 0.30, p < 0.01) (Fig. 1a, b). Besides, ROC curve analysis indicated that SYT8 has good diagnostic value for CRC (AUC = 0.836, 95% CI: 0.787−0.886), with an optimal cut-off value of 0.559 (sensitivity 70.63%, specificity 86.28%) (Fig. 1a, b).
Table 1. Correlation analysis of clinicopathologic parameters and expression of SYT8.
Characteristics Total Low expression of SYT8 (%) High expression of SYT8 (%) p-value n 644 322(50) 322(50) Gender, n (%) 0.477 Female 301 155 (51.5) 146 (48.5) Male 343 167 (48.7) 176 (51.3) Race, n (%) 0.649 White 313 175 (55.9) 138 (44.1) Asian and black or African American 81 43 (53.1) 38 (46.9) Unknown 250 104 (41.6) 146 (58.4) Age, n (%) 0.633 ≤ 65 276 141 (51.1) 135 (48.9) > 65 368 181 (49.2) 187 (50.8) Pathologic T stage, n (%) 0.046 T1 & T2 131 55 (42) 76 (58) T3 & T4 510 264 (51.8) 246 (48.2) Unknown 3 3 (100) 0 (0) Pathologic N stage, n (%) 0.767 N0 368 181 (49.2) 187 (50.8) N1 & N2 272 137 (50.4) 135 (49.6) Unknown 4 4 (100) 0 (0) Pathologic M stage, n (%) 0.107 M0 475 228 (48) 247 (52) M1 89 51 (57.3) 38 (42.7) Unknown 80 43 (53.7) 37 (46.3) BMI, n (%) 0.358 ≤ 25 107 54 (50.5) 53 (49.5) > 25 222 124 (55.9) 98 (44.1) Unknown 315 144 (45.7) 171 (54.3) CEA level, n (%) 0.279 ≤ 5 261 128 (49) 133 (51) > 5 154 84 (54.5) 70 (45.5) Unknown 229 110 (48) 119 (52) Values in bold are statistically significant. 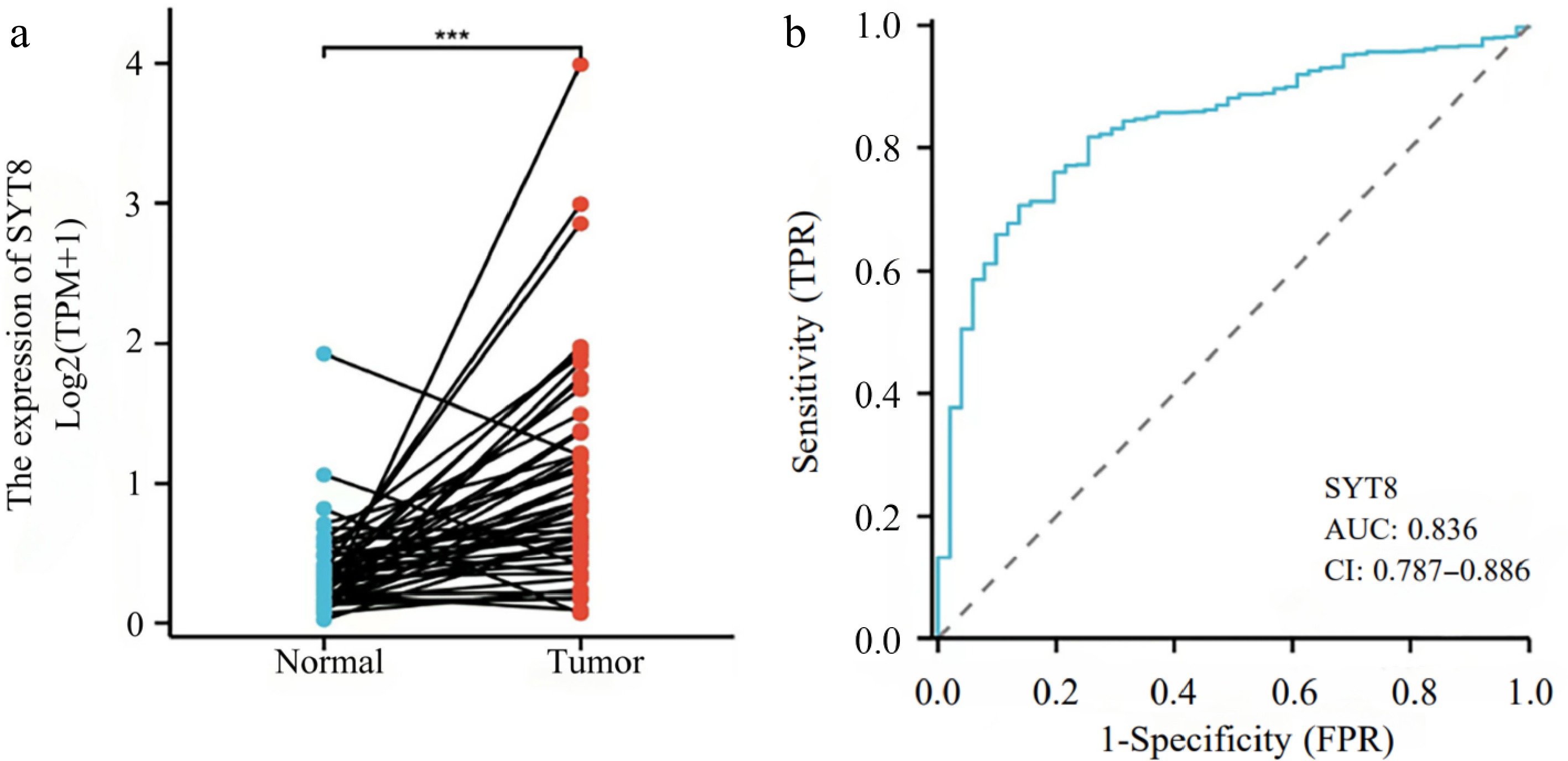
Figure 1.
Expression and diagnostic role of SYT8 in CRC. (a) SYT8 expression assessed by Wilcoxon signed rank test. (b) Diagnostic value analyzed by ROC curve.
Prognostic significance of SYT8 expression in CRC patients from the TCGA dataset
-
To further evaluate the performance of SYT8 to predict outcomes in CRC patients, we conducted Kaplan-Meier and Cox regression analyses. The Kaplan-Meier analysis demonstrated that patients with high SYT8 expression had significantly worse PFI and OS (p < 0.05, Fig. 2a, b). Meanwhile, the results of online analysis using the Kaplan-Meier Plotter database showed that OS and PFS in the SYT8 low expression group were significantly higher than those in the SYT8 high expression group (Fig. 3a, b). Therefore, we hypothesized that SYT8 high expression may be one of the factors for poor prognosis in patients with colorectal cancer.
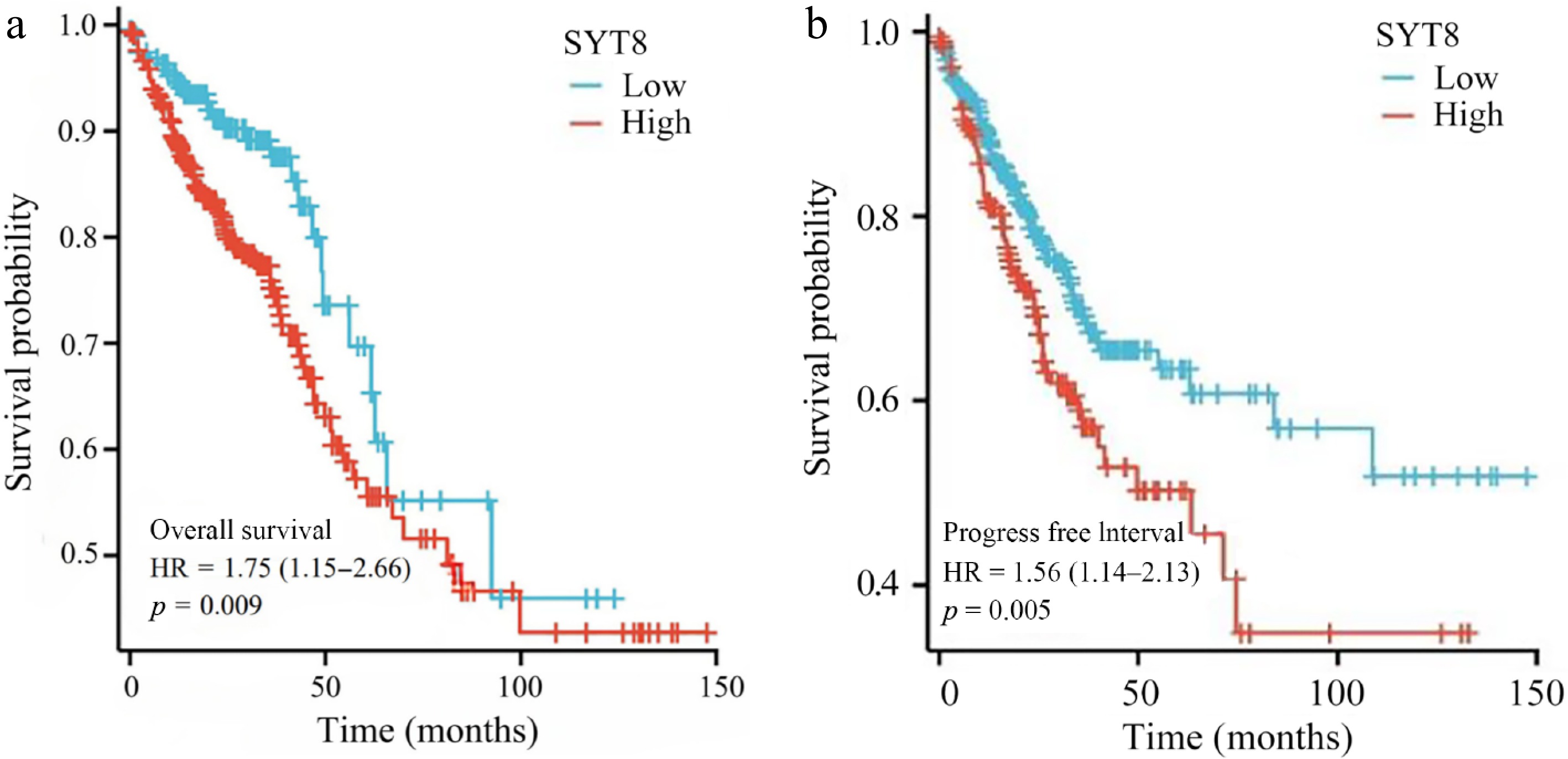
Figure 2.
Survival analysis assessed by Kaplan-Meier analysis. (a) The SYT8-high group was more likely to have a worse overall survival compared with that of the SYT8-low group. (b) The SYT8-high group was more likely to have a worse progress free interval compared with that of the SYT8-low group.
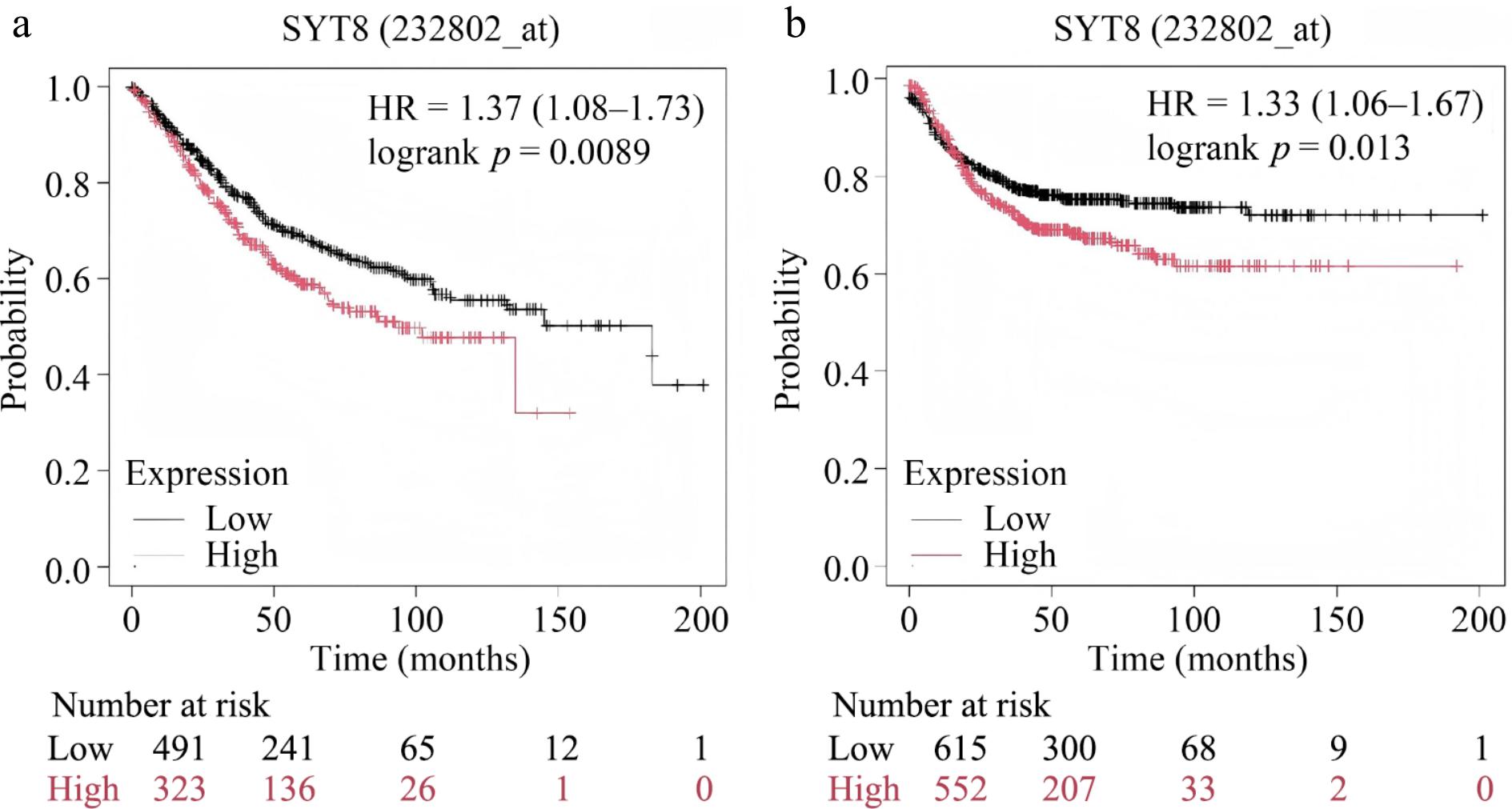
Figure 3.
Survival analysis based on the Kaplan-Meier Plotter database. The Kaplan-Meier curves of patients with SYT8 high expression and SYT8 low expression are shown. (a) OS. (b) PFS.
In the multivariate analysis, SYT8 expression was identified as an independent prognostic factor for poor OS (p = 0.01), but not for PFI (Tables 2 & 3). Moreover, age (p < 0.001), T stage (p = 0.004), lymph node involvement (p = 0.009), and distant metastasis (p < 0.001) were also found to be independent prognostic indicators of OS in CRC patients.
Table 2. COX regression analysis to assess prognostic factors for PFI.
Characteristics Total (N) Univariate analysis Multivariate analysis Hazard ratio (95% CI) p Hazard ratio (95% CI) p Gender (male/female) 643 1.217 (0.892−1.660) 0.216 Race (Asian and black or African American/white) 394 1.547 (0.992−2.412) 0.054 1.322 (0.807−2.168) 0.268 Age (> 65/≤ 65) 643 1.006 (0.737−1.371) 0.972 Pathologic T stage 640 T1 & T2 131 Reference Reference T3 & T4 509 3.198 (1.814−5.636) < 0.001 2.073 (0.871−4.933) 0.099 Pathologic N stage 639 N0 367 Reference Reference N1 & N2 272 2.624 (1.916−3.592) < 0.001 0.963 (0.591−1.570) 0.881 Pathologic M stage (M1/M0) 563 5.577 (3.945−7.884) < 0.001 6.018 (3.596−10.069) < 0.001 SYT8 (high/low) 643 1.135 (0.836−1.541) 0.418 Values in bold are statistically significant. Table 3. COX regression analysis to assess prognostic factors for OS.
Characteristics Total (N) Univariate analysis Multivariate analysis Hazard ratio (95% CI) p Hazard ratio (95% CI) p Gender (male/female) 643 1.054 (0.744−1.491) 0.769 Race (Asian and black or African American/white) 394 1.072 (0.622−1.848) 0.802 Age (> 65/≤ 65) 643 1.939 (1.320−2.849) < 0.001 2.583 (1.667−4.002) < 0.001 Pathologic T stage 640 T1 & T2 131 Reference Reference T3 & T4 509 2.468 (1.327−4.589) 0.004 2.277 (1.034−5.011) 0.041 Pathologic N stage 639 N0 367 Reference Reference N1 & N2 272 2.627 (1.831−3.769) < 0.001 1.842 (1.164−2.916) 0.009 Pathologic M stage (M1/M0) 563 3.989 (2.684−5.929) < 0.001 3.105 (1.949−4.948) < 0.001 SYT8 (high/low) 643 1.356 (0.956−1.923) 0.087 1.666 (1.130−2.455) 0.010 Values in bold are statistically significant. Clinicopathological features of CRC patients in the retrospective validation cohort
-
To corroborate these findings, we analyzed 153 postoperative CRC patients. IHC staining results indicated that SYT8 expression was scarcely detectable in adjacent tissues, while the intratumoral positive rate was 38% (58/153) (Fig. 4a−c). Specifically, our analysis demonstrated that patients with high SYT8 expression were significantly associated with lymph node metastasis (p = 0.008). However, no significant correlations were discovered between SYT8 expression and age (p = 0.386), gender (p = 0.64), margins (p = 0.201), vascular invasion (p = 0.192), nerve invasion (p = 0.221), T stage (p = 0.283), distant metastasis, or differentiation (p > 0.05) (Table 4).
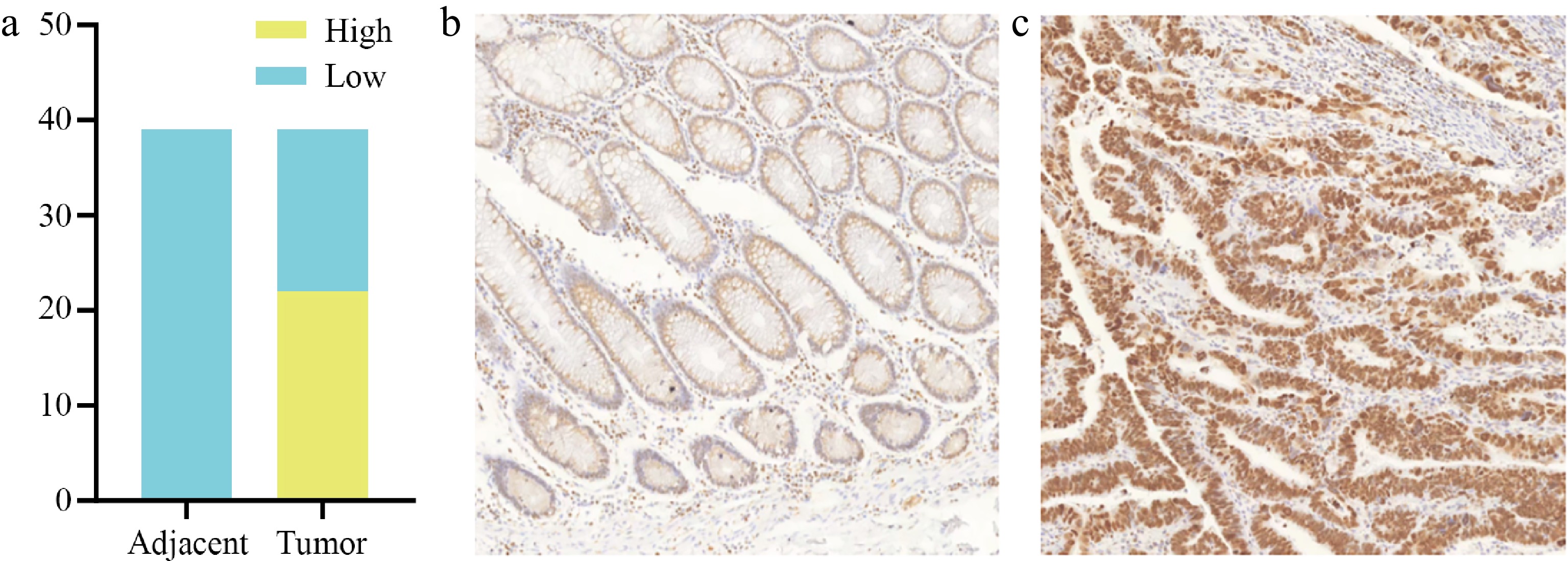
Figure 4.
SYT8 expression in tumor tissues and adjacent tissues of CRC patients. (a) SYT8 expression levels in CRC tissues was higher than adjacent tissues. (b) Immunohistochemical images of CRC adjacent tissue with low SYT8 expression. (c) Immunohistochemical images of CRC adjacent tissue with high SYT8 expression.
Table 4. Clinicopathologic parameters and demographic features in CRC patients with or without SYT8 expression in the retrospective validation cohort.
Characteristics Total Positive Negative P value n 153 58(38) 95(62) Age, n (%) 0.386 ≥ 60 58 37(63.8) 21(36.2) < 60 95 67(70.5) 28(29.5) Gender, n (%) 0.64 Male 94 37(39.4) 57(60.6) Female 59 21(35.6) 38(64.4) Margins 0.201 Present 1 1(100) 0(0) Absent 152 57(37.5) 95(62.5) N stage 0.008 N1 74 36(48.6) 38(51.3) N0 79 22(27.8) 57(72.2) Vascular invasion 0.192 Present 56 25(44.6) 31(55.4) Absent 97 33(34) 64(66) Nerve invasion 0.221 Present 49 22(44.9) 27(55.1) Absent 104 36(34.6) 68(65.4) T stage 0.283 T1 2 0(0) 2(100) T2 11 3(27.3) 8(72.7) T3 122 45(36.9) 77(36.1) T4 18 10(55.6) 8(44.4) Differentiation 0.41 Low 34 16(47.1) 18(52.9) Middle 108 39(36.1) 69(63.9) High 11 3(27.3) 8(72.7) M stage 0.571 M1 5 3(60) 2(40) M0 148 55(37.2) 93(62.8) Values in bold are statistically significant. Prognostic role of SYT8 in CRC patients in the retrospective validation cohort
-
The Kaplan-Meier analysis indicated that patients exhibiting high SYT8 expression experienced inferior DFS and OS outcomes (p < 0.05, Fig. 5a, b). Multivariate analysis results demonstrated that increased SYT8 expression and distant metastasis were independent prognostic factors for poor OS (Table 5). Nevertheless, no statistically significant correlation was identified between SYT8 expression and DFS in CRC patients, with distant metastases being the sole prognostic factor for poor DFS (Table 6).
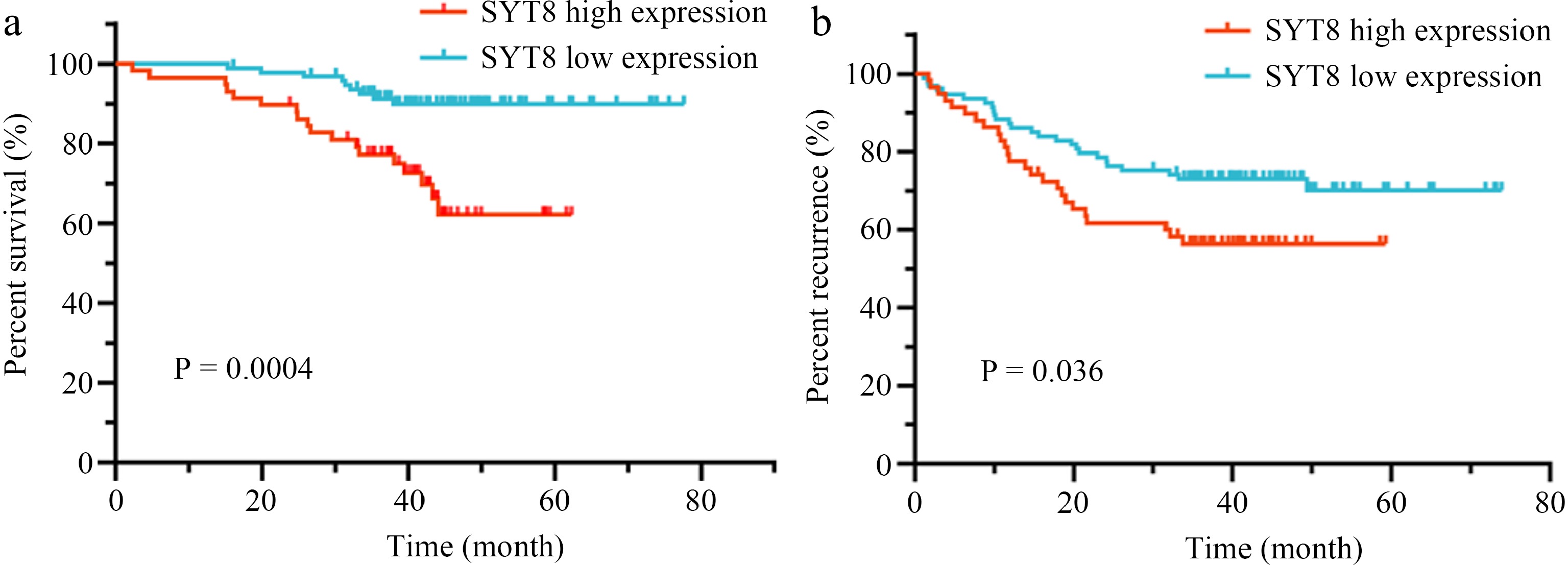
Figure 5.
Survival analysis assessed by Kaplan–Meier analysis in the retrospective validation cohort. (a) The SYT8-high group had a worse overall survival compared with that of the SYT8-low group. (b) The SYT8-high group had a worse disease free survival compared with that of the SYT8-low group.
Table 5. COX regression analysis to assess prognostic factors for OS in the retrospective validation cohort.
Characteristics Univariate analysis Multivariate analysis Hazard ratio (95% CI) p Hazard ratio (95% CI) p SYT8 (low/high) 3.811 (1.710−8.494) 0.001 3.256 (1.427−7.426) 0.005 Gender (male/female) 1.265 (0.568−2.815) 0.561 Age (≥ 60/< 60) 2.006 (0.759−5.298) 0.160 N stage (N1/N0) 1.460 (0.683−3.120) 0.329 M stage (M0/M1) 0.139(0.041−0.467) 0.001 0.150 (0.042−0.532) 0.003 Margins (absent/present) 0.047 (0.006−0.384) 0.004 Vascular invasion (absent/present) 0.405 (0.190−0.867) 0.020 Nerve invasion (absent/present) 0.376 (0.177−0.802) 0.011 T stage 0.035 T1/T4 0.980 T2/T4 0.166 (0.020−1.357) 0.094 T3/T4 0.286 (0.119−0.684) 0.005 Differentiation 0.197 Low/high 1.534 (0.331−7.108) 0.584 Middle/high 0.723 (0.166−3.145) 0.665 Values in bold are statistically significant. Table 6. COX regression analysis to assess prognostic factors for DFS in the retrospective validation cohort.
Characteristics Univariate analysis Multivariate analysis Hazard ratio (95% CI) p Hazard ratio (95% CI) p SYT8 (low/high) 1.790 (1.031−3.108) 0.039 1.571 (0.891−2.770) 0.119 Gender (male/female) 1.246 (0.696−2.230) 0.459 Age (≥ 60/< 60) 1.623 (0.833−3.164) 0.155 N stage (N1/N0) 1.723 (0.986−3.011) 0.056 M stage (M1/M0) 4.603 (1.643−12.892) 0.004 3.713 (1.304−10.574) 0.014 Margins (absent/present) 0.143 (0.019−1.064) 0.057 Vascular invasion (absent/present) 0.805 (0.461−1.407) 0.447 Nerve invasion (absent/present) 0.523 (0.300−0.910) 0.022 T stage 0.068 T1/T4 T2/T4 0.111 (0.014−0.870) 0.036 T3/T4 0.466 (0.233−0.932) 0.031 Differentiation 0.217 Low/high 0.989 (0.325−3.011) 0.985 Middle/high 0.594 (0.210−1.678) 0.326 Values in bold are statistically significant. -
To assess the diagnostic and prognostic value of SYT8 in GC patients who received curative surgery, we analyzed differential gene expression and conducted Kaplan-Meier analyses utilizing TCGA datasets. Our findings indicated a remarkable diagnostic significance in CRC, while patients exhibiting high SYT8 expression demonstrated poor PFI and OS. To verify these results, we retrospectively analyzed CRC patients who had received curative surgery at our center. We observed significantly higher SYT8 expression levels in CRC tissues compared to adjacent tissues, with increased SYT8 expression strongly correlating with lymph node metastasis. Further Kaplan-Meier and multivariate analyses demonstrated that patients with low SYT8 expression in tumor tissues had a lower risk of disease recurrence and mortality compared to those with high expression. Moreover, distant metastasis and high SYT8 expression were identified as independent prognostic factors influencing patient survival. These findings aligned with the significance of SYT7, another member of the SYT family, which has been demonstrated to be overexpressed in CRC tissue and associated with advanced staging[13]. Previous research has indicated that SYT8 may play a crucial role in gastrointestinal malignant tumors. Kanda et al.[11] clarified that high SYT8 expression was significantly associated with peritoneal metastasis and could be applied as an independent prognostic marker for peritoneal recurrence-free survival in stage II/III GC patients. In addition, SYT8 may affect the sensitivity of GC cells to 5-FU.
Our study is the first to explain the clinicopathological and prognostic significance of SYT8 in CRC. Nevertheless, the underlying mechanisms by which SYT8 influences patient outcomes in CRC remain less understood. Synaptotagrin (SYT), a transmembrane protein, plays a crucial role in neurotransmission and hormone secretion, while also influencing malignant tumor cell behavior. Previous research[14] has demonstrated that SYT8 levels were upregulated in pancreatic cancer tumors, contributing to increased cell proliferation, migration, and invasion in both in vitro and in vivo studies. This effect was attributed to the TNNI2/ERRα/SIRT1 signaling pathway. Moreover, numerous studies have demonstrated that SYT family molecules involved in carcinogenesis and modulation of the immune infiltration microenvironment[15−17].
The incidence and progression of CRC are closely associated with abnormal protein expression, suggesting that certain proteins could be applied as valuable diagnostic biomarkers and therapeutic targets[18−20]. Our research identified SYT8 as a potential diagnostic and prognostic biomarker in CRC patients. These findings may aid in identifying high-risk patients based on SYT8 expression, thereby enabling more accurate clinical management. If SYT8 is overexpressed, it may indicate poor response to treatment and poor prognosis. In terms of treatment, the detection results of SYT8 indicators can provide a reference for doctors to choose treatment options. For patients with lymph node metastasis, the expression level of SYT8 can be positively detected. If SYT8 is highly expressed, closer follow-up is needed after surgery, and doctors may choose more active treatment options. Although there is no specific treatment drug, chemotherapy, radiotherapy, targeted therapy, immunotherapy, and other methods can be considered comprehensively. In addition, SYT8 has higher specificity and sensitivity in evaluating the prognosis of patients with CRC compared to carcinoembryonic antigen (CEA) and carbohydrate antigen 19-9 (CA19-9). SYT8 can be used in combination with traditional tumor markers to evaluate the prognosis of patients and guide treatment. In this study, we first reported the clinicopathological role of SYT8 in CRC patients and evaluated its diagnostic and prognostic significance. However, several limitations should be noted. First, this retrospective study has a limited sample size and offers a modest level of evidence. Besides, all included CRC patients were Chinese, potentially limiting the applicability of our results to other populations. Finally, extended follow-up is necessary to obtain more robust endpoints.
In conclusion, our research offers a rigorous analysis of the diagnostic and predictive value of SYT8 in CRC patients, indicating a significant correlation between its expression and lymph node invasion and metastasis.
-
This study was approved by the Research Ethics Committee of Affiliated Hospital of Nanjing University of Chinese Medicine (NO.2022NL-137-01). Informed written consents were collected from all the eligible patients and the entire study was conducted in accordance with the principles outlined in the Helsinki Declaration.
Our research was supported by grants from Jiangsu Province Graduate Student Research and Practice Innovation Program (SJCX24_0944), Jiangsu Provincial Medical Key Discipline (Laboratory) (No. ZDXYS202208).
-
The authors confirm contribution to the paper as follows: study conception and design, analysis, and interpretation of results: Zhu J, Shang J; data collection: Li Y; draft manuscript preparation: Bai L, Kulabiek D; guidance and support: Zheng X, Zhang Y, Qiao J. All authors reviewed the results and approved the final version of the manuscript.
-
The data that support the findings of this study are available from the corresponding author upon reasonable request.
-
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations or those of the publisher, editors, and reviewers. Any product that may be evaluated in this article or claim that may be made by the manufacturer is not guaranteed or endorsed by the publisher.
-
# Authors contributed equally: Jin Zhu, Jiarong Shang
- Copyright: © 2025 by the author(s). Published by Maximum Academic Press, Fayetteville, GA. This article is an open access article distributed under Creative Commons Attribution License (CC BY 4.0), visit https://creativecommons.org/licenses/by/4.0/.
-
About this article
Cite this article
Zhu J, Shang J, Li Y, Kulabiek D, Bai L, et al. 2025. Clinicopathological features and prognostic significance of SYT8 in patients with colorectal cancer who received curative surgery. Gastrointestinal Tumors 12: e005 doi: 10.48130/git-0025-0005 

Clinicopathological features and prognostic significance of SYT8 in patients with colorectal cancer who received curative surgery
- Received: 08 October 2024
- Revised: 14 January 2025
- Accepted: 13 February 2025
- Published online: 27 March 2025
Abstract: To clarify the clinicopathological and predictive significance of SYT8 expression in patients with colorectal cancer (CRC) who underwent radical tumor resection. The demographic, clinicopathologic, survival outcomes, and SYT8 expression information in CRC patients were extracted from The Cancer Gene Atlas (TCGA) databases. Then we assessed the diagnostic value of SYT8 and determined the underlying prognostic factors of PFI and OS. The SYT8 core genes were identified online based on the Kaplan-Meier Plotter database, and prognostic information was obtained for online analysis. To validate the above results, we retrospectively analyzed 153 CRC patients, and collected their clinicopathological, demographic, and survival information. The clinicopathological features and prognostic value of SYT8 were analysed in patients with colorectal cancer. In total, 643 CRC patients were included from the TCGA database. SYT8 was significantly overexpressed in CRC tissues compared to adjacent tissues (0.84 ± 0.79 vs 0.28 ± 0.30, p < 0.01). ROC curve results indicated that SYT8 performed a satisfactory diagnostic value in CRC (AUC: 0.863). Additionally, SYT8 was an independent prognostic factor affecting patients' OS (p = 0.01) instead of PFI. The results of retrospective validation demonstrated that SYT8 expression is one of the independent prognostic factors to OS (p < 0.05). Moreover, SYT8 expression was positively correlated with lymph node metastasis. SYT8 overexpressed in CRC tissues and could be applied as a diagnostic and prognostic biomarker in these patients after curative surgery.
-
Key words:
- Colorectal cancer /
- SYT8 /
- Prognosis /
- Retrospective analysis